A New Future of Healing Environment
Evidence-based DesignIntroduction
For the past decades, the concept of healing environment has settled like the Holy Grail in the design of healthcare facilities. Derived from the idea that the healthcare facilities designed by architects serve not only as the background of medical treatment but also as an important coordinator in the process of treating patients, this concept became grafted with "patient-centered care" which emerged under the leadership of American nonprofit organizations like Planetree or the Picker Institute. Consequentially engendering a new form of hospitals that escaped from the past form based on mechanical functions, the concept of healing environment constitutes one of the important paradigmatic changes in the history of hospital design, providing architects with the golden chances of experimenting with their own creativity.
In Korea, however, the concept of healing environment has been losing its original vitality. Although it is always mentioned as one of the design purposes for all hospital projects, healing environment is interpreted by designers too arbitrarily without a concrete criterion or conceptual development so as to fall into a cliche which can no longer give a true sense of purpose to architects. By the way, the same concept is recently evolving into a new phase, the emergence of evidence-based design (EBD). Today, EBD is inspiring vitality in the hackneyed phrase by increasing the conceptual width and depth of healing environment and suggesting a new goal towards which hospital design should advance.
The Concept and Background of Evidence-based Design

According to the Center for Health Design, an American non-profit organization leading the research, education, and propagation of evidence-based design, EBD can be described as the "judicious endeavor to base every decision process of design on the best evidence available presently," and its purpose as "not only to improve the outcome, but also to monitor its success or failure so as to apply it for the next decision process." The concept of EBD was borrowed from that of evidenced-based medicine (EBM) in healthcare. That is, the concept of EBM as the "conscientious, explicit, and judicious use of modern, best evidence" was applied to the hospital design as it is in making decisions about the care of patients, along with the knowledge and experience of individual doctor. EBD can be seen as the product of reflecting on the existing concept of healing environment. This is to say that such plenty of projects attempted under the banner of so-called healing environment have not all been effective unlike their intents despite the steady development of hospital design for the past decades.
On the other hand, EBD may also seen as that which evolved from healing environment. The findings of connection between the physical environment and the treatment result have been steadily piled up, so that architects came to have wide access to such objective data. Hospital design—particularly, amongst general building design—requires highly organizational and interdisciplinary knowledge fit for its professional and complex nature. A close look at the actual design process, however, often reveals the reality in which the limited knowledge and experience of a few lead designers serve as the main grounds of design decision.
If architecture is the combination of art and science, EBD may well be an endeavor to recover the equilibrium by balancing the existing convention of arbitrarily biased design decision with rationality and objectivity.
The Research and Application Trends of EBD
There are plenty of research evidencing that hospital design and clinical outcomes are closely related. Roger S. Ulrich's paper published in 1984 is often discussed as the first research on EBD. In the research titled "View through a Window May Influence Recovery from Surgery," he reported that patients assigned to rooms with windows recovered sixteen hours earlier on average than those who were not. After this landmark research, there have reportedly been a pile of various research on EBD amounting to about 1,200 works by 2008. Unlike the conventional intent-based design reliant upon individual intuitions and experiences, EBD aims at presenting design outcomes improved practically by systematic combination between design decision process and existing research findings. The practical improvement here means the amelioration of objective indexes like nosocomial (acquired-in-hospital) infection, cases of inpatient falls, patient recovery speed, and surveyed patient satisfaction.
The application of EBD in the US came into full bloom with the Pebble project, which began in 2000 under the leadership of the aforementioned Center for Health Design. About twenty hospitals which firstly participated to set out this project applied EBD to the new construction, repair, and maintenance works. Then shared and reviewed, the amelioration effects by EBD application proved more significant than ever. By and large, there are more than fifty hospitals participating in this project now. Another case similar with this Pebble project is the Fable Hospital project, which was to newly construct a hospital that would replace the existing hospital, with a capacity of three hundred beds. Amongst the various principles of EBD applied to this project, notable is the installation of so-called acuity-adaptable units for all wards. This took additional costs of 12 million dollars, which were about 5% of the initial investment and almost of which, including such an indirect effect as the increase of market share, were disinvested within a year. As the effects of EBD began to be visualized in this way, its application gradually became essential for designing healthcare facilities in the US.
A recent questionnaire survey with 40 architectural firms in the US revealed that 37 firms out of them were applying EBD, and the Military Health System of the US Department of Defense established a guide to apply the concept of "patient-centered" care and the principles of EBD for all healthcare facility projects. EBD was also settled as the core methodology of healthcare facility design by a number of profit or nonprofit healthcare organizations including Kaiser. EBD is not so much a theory itself, but an attitude and principle. This principle can be applied to any design field. It is recently being applied not only to hospitals or research institutes, but also to schools, offices, penitentiaries, and houses, as well as widely to urban or interior designs.
The Elements of EBD

EBD largely breaks into two elements: patient-centeredness and patient-safety. If the former is the core of the past "healing environment" concept, the latter belongs to the extension of the same concept. First, the patient-centeredness begins with the concept of patient-centered care. Already familiar to us, this element is an endeavor to protect the dignity of patients from the unfamiliar environment of hospital so as to relieve their stress, i.e. to make stress-free environment: specifically, it focuses on patients' privacy issues such as managing patient information, controlling visual and auditory physical environment, securing territoriality, resolving congestion, as well as the right to environmental control and choice, social exchange and support, way-finding, healing effects of natural elements, positive distraction, and the like.
The importance of this element can be intuitively affirmed by anyone, but it is difficult to control its variables and so quantifiably verify the result of hospital design. For all that, research on EBD made it possible to verify what we had only intuitively understood, thus broadening our understanding of this element. Meanwhile, new counter-evidences against our preconceptions are also emerging. For example, the previous convention was to focus on unconditional elimination of stimulus factors to reduce the patients' stress, while a recent study suggests that a certain degree of stimulus is necessary to avoid ennui and mental numbness. Also, the communication with other patients regarded as one of the advantages of multi-bed rooms became discredited as it proved that other patients in the same room rather tend to be the cause of stress.
For the orientation of wards, southern orientation has been mainly preferred in Korea, but a recent study on EBD found that the morning sunlight has good effects of treating seasonal affective disorder (SAD) or melancholia. Accordingly, a new trend is emerging that emphasizes the importance of east-oriented wards.
Second, the patient-safety element had been overlooked until its importance was newly emphasized by EBD. "First, do no harm (Primum non nocere)": this concept originated from Hippocrates was taken by Nightingale, and ultimately appeared at the first part of the Guidelines for Design and Construction of Health Care Facilities published by the Facility Guidelines Institute. The patient safety is also the keyword of the Joint Commission International Accreditation Standards, the international certification system for healthcare facilities by which Korean healthcare organizations are competitively attempting to be credited.
The elements about patient safety include infection control, air quality improvement, inpatient fall prevention, medical error prevention, and noise control. For infection control, it was reported that the cases of nosocomial infection in the US reach about 2 million persons (a twentieth of all inpatients), and 80 to 90 thousand persons die every year from the infection. One can find that nosocomial infection was obviously resolved just with hand washing: in case of St. Joseph Medical Center, changing the design of the intensive care unit and the location of washbowls was reported to have reduced nosocomial infection by as much as 44%.
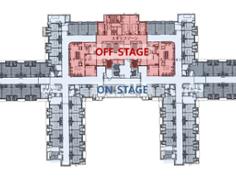
For medical error prevention, the past paradigm "The system has no problem; blame the blunderer" has changed into "Any person could make an error; change the system." That is to say, the paradigm has shifted in such a way as to ameliorate the environment and so prevent errors from occurring. A case in point here is the standardization of rooms, which is to reduce the potential occurrence of errors by standardizing healthcare instruments, appliances, utility layout, and the like, so as for the medical staff to intuitively and efficiently use them. This is related to such design strategies as modularization of outpatient clinic layout, universal operating room, same-handed design, and acuity-adaptable unit.
What is most actively researched and designed in EBD is the ward which includes the intensive care unit. The present U.S. system is taking single-bed rooms as normal. Except for the cost, single-bed rooms are better than multi-bed rooms in all the aspects of patient treatment such as infection control, patient privacy, environmental control and choice, family participation, and communication with the medical staff. Additionally, the United States is adopting acuity-adaptable units, which necessitate Not surprisingly, the U.S. healthcare system is going so far as to adopt the "acuity-adaptable unit," which enables patients to stay there throughout the duration with no need to change the room from the intensive care unit through the sub-intensive care unit to the general ward. In this case, a report evidences, the movement of patients is reduced by 90%, so that the number of inpatient falls is reduced by 75%.
Domestic Application of EBD

Be it a concept of "reflection" or "development" of healing environment, EBD has been a mainstream concept in American hospital architecture since about a decade ago. Also, it has been accepted not just as one of the methodological trends of hospital design, but as one of the best practices to achieve the best outcome in various design fields. In Korean hospital architecture, however, the discussion of EBD has been only at a minimal level. Even worse, research is lacking on the feasibility of applying EBD, such as the aforementioned total single-bed policy, to this country's healthcare whose policy and reality are different from those of foreign countries, while most existing studies are from the Western academy revolving around the North America.
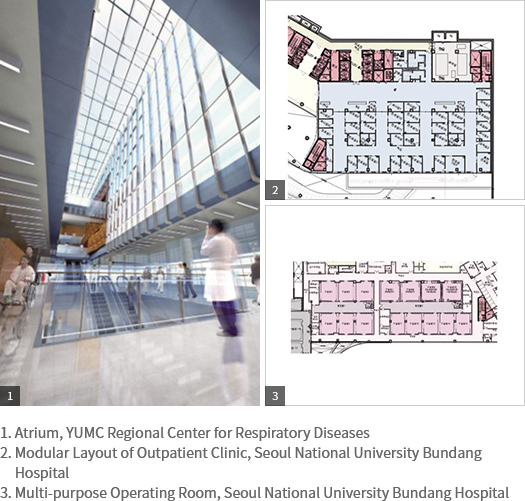
The hospital design team of Junglim Architecture has applied EBD at least partially to projects since about 2005, taking the lead of introducing the concept in this country by having in-house training sessions and lectures outside to publicize it. For the 2009 extension project of Seoul National University Bundang Hospital, we applied EBD as a design methodology from the initial phase. Afterwards, it has served as a foundation to develop the hospital design methodology of Junglim Architecture. We applied the modular layout of outpatient clinic, multi-purpose operation rooms, infection control augmentation, and the same-handed design for single-bed and two-bed rooms to SNU Bundang Hospital, probably the first hospital in this country which was designed and built in reality with active application of EBD. Be that as it may, in order to prevent the future of EBD from degenerating into a vacant cliché that decorates design reports just as the past concept of "healing environment" did, we should continue to make efforts to review and implement the hitherto research findings which have persisted around but been overlooked. A good example that shows such efforts are not impossible is the very recent "sustainable architecture," which cannot help but become "evidence-based" fundamentally because one cannot convince the project owner only in the name of environment-friendliness without any concrete evidence on results or efficiencies.
Conclusion: the Future of EBD
The future clients of hospital projects will demand the apparent performances and efficiencies of buildings to they invest in. They will request designers a set of tasks and want to verify whether it really functions or not after completion, that the building should be safe for patients, serve for treatment performance, have good efficiency of spatial use, satisfy patients and the medical staff in using it, save the maintenance fee and raise the operation efficiency, and the like. Indeed, we should ask ourselves whether or not we are really prepared for these all.
Our journey to discover the Holy Grail of "healing environment." Unlike the previous ambiguous journey, however, EBD is shedding light more vividly to our way ahead. Just like the American Pebble project, we hope this "evidence-based design" will become widespread as if a pebble cast into the pond makes ripples spread gradually.
Reconstructed Excerpts from "Ruminating Upon the Basics of Junglim Architecture," Junglim Architecture Works 2013